Role
IA Program lead @ Doctolib Connect
Duration
6 months
Industry
HealthTech
Responsibility
Research & Discovery
Integration Strategy
Management & Prioritization
Design & Buy-in
Workshop Facilitation
Team
Product Director
Head of Design
User Researcher
Data Analyst
2x Account Managers
TL;DR
Doctolib acquired Siilo (now Doctolib Connect) to scale clinical collaboration. Two years post-acquisition, adoption was at 10% and the products remained siloed. I identified this as an architecture problem, not a feature problem, and initiated and led a cross-functional IA program to restructure how collaboration works across products, teams, and markets.
+15%
Care team messaging activation
+20%
Contact sync adoption
70%
WAU for new organizations
with 5-35 members
Shared
collaboration layer across the company
Disclaimer: Confidential information has been omitted or obfuscated. This case reflects my own perspective and not necessarily the views of Doctolib.

Context
Doctolib acquired Siilo (Now Connect), But integration didn't happen!
The vision was to combine Doctolib's clinical tools with Europe's Largest Clinical Messaging tool, into one seamless experience. Two years later, most Doctolib users never touched Connect, and most Connect users saw no improvements.
Objective
Make the org aligned, and re-Position Connect inside and outside
I proposed an Information Architecture program to the Product Director, Head of Design, and Head of Engineering, and got the mandate to lead it.
My bet
If we restructure the underlying logic of clinical collaboration before shipping more features, we could stop teams from building in siloes.
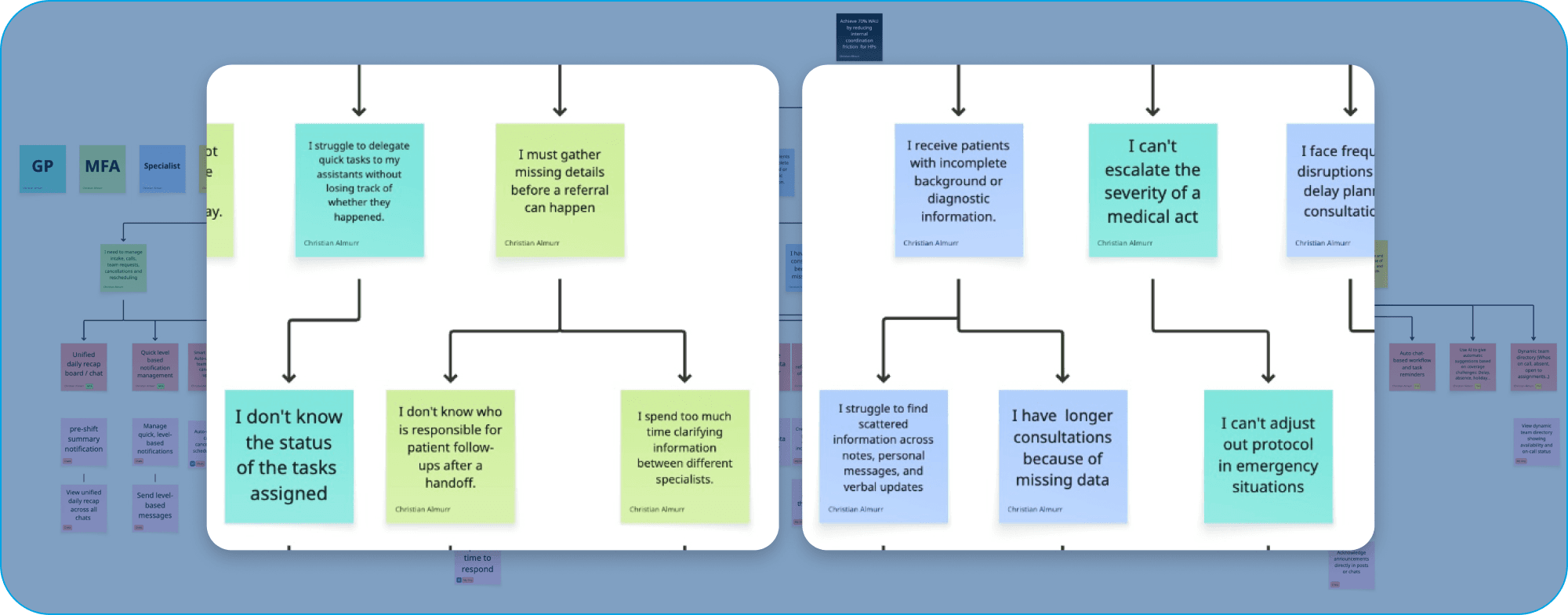
I deprioritized our most active client; Small practices
After the first discovery cycle, I saw that large organizations carry the structural complexity that would break our architecture if left unaddressed.
Small practices run linear workflows so they'd benefit downstream. I made the call to solve the harder architecture first and scale down, not up. This was contested internally.

Strategy hypothesis: Connect the 2 main pillars of the CC&C industry (Clinical Communication & Collaboration) along with Connect's USP to build the best Communication & Collaboration platform in Europe

Initial vision design vision for the Mobile app.

My Messages Section Architecture explorations with David B. and Felix T.
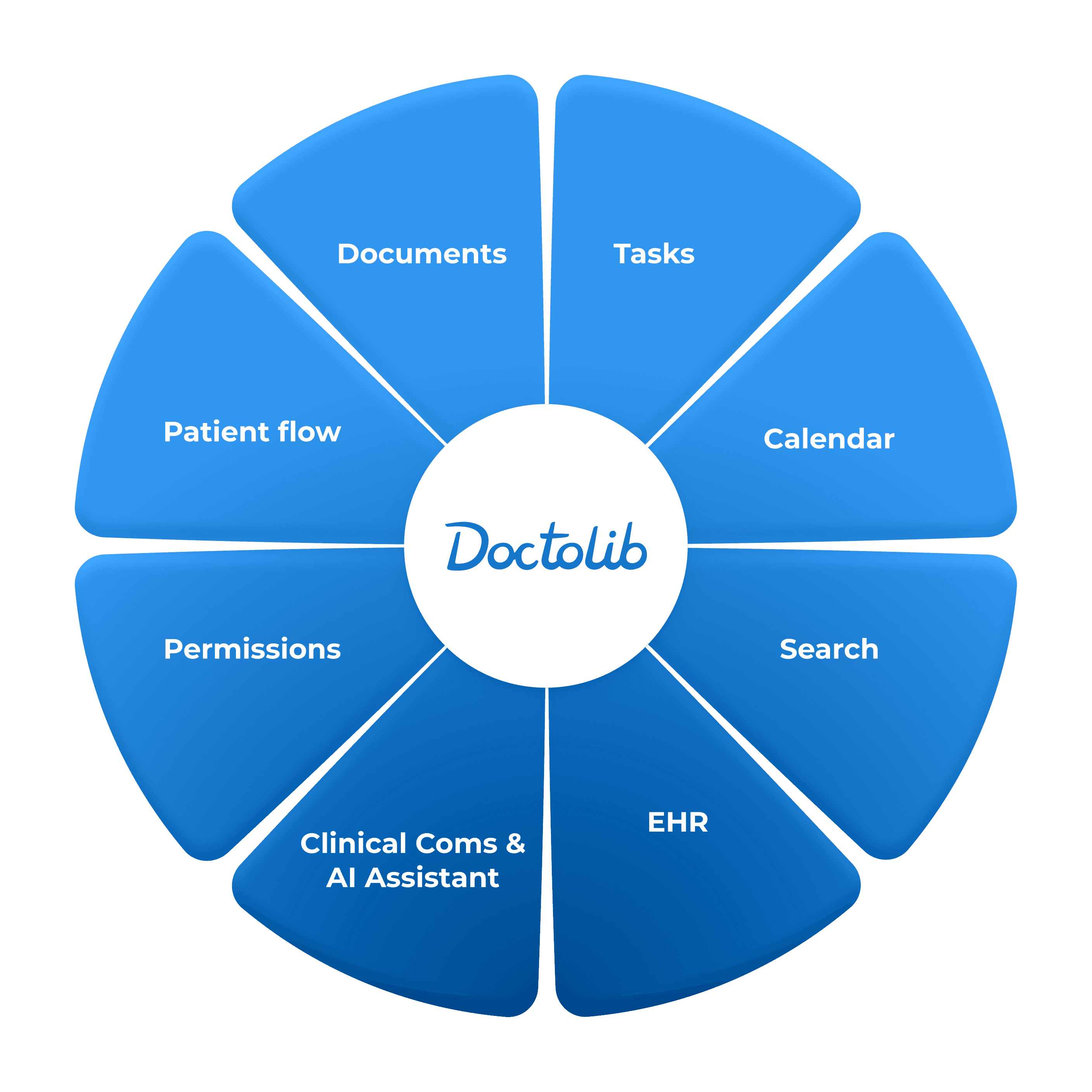
System
A horizontal product domain that connects tools together and leverages network Effects
I worked with the Design team to setup 3 design principles and 7 beliefs that now govern design decisions across product teams. Some of those included:
Think mobile, design desktop
Clinical collaboration happens between rooms and shifts, not at a desk. We think mobile-fist, design desktop-first.
Build collaboration in collaboration
Embed with their other teams early on, co-design the integration points, and setup success metrics on both sides of the integration
Design with confidence
User confidence is the foundational lever. If professionals don't trust the system, adoption dies regardless of functionality. I made it a structural principle, not a polish pass. Read more about my research
From D.Connect as a separate domain
Doctolib Connect was treated as messaging tool, separate from other tools, teams, and patient contexts.
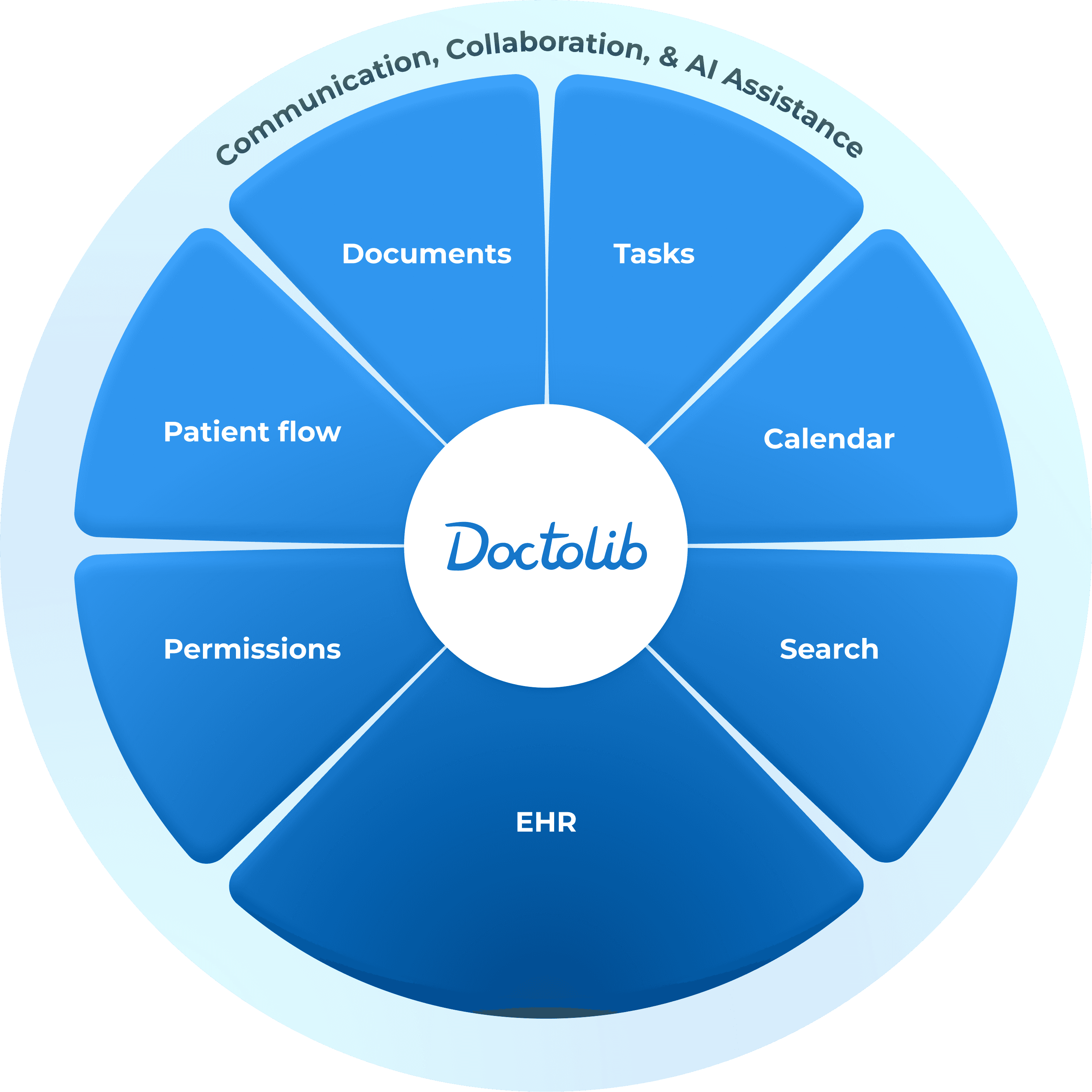
To Connect as a Horizontal Layer
Doctolib Connect became a collaboration system. Messaging enable shared context, and responsibilities.


Impact
Care teams became more active. Product teams aligned without Friction.
Ongoing experiments to mobilize the system validated the direction:
+15% Care Team Messaging activation
+20% contact sync adoption
70% WAU for newly registered organizations that have 5–35 users
The larger impact
Product teams stopped building overlapping features. The IA initiative gave engineering, product, and GTM a shared structure for where Connect fits, reducing rework and setting a foundation for CareCo's expansion roadmap.

Validated UI annotations
Learnings
Strategic design means containing ambiguity, not resolving it
Sustainable scalability can only be achieved by containing uncertainty so teams can move without constant redesign. Invest earlier in alignment rituals: smaller narrative tests, clearer tradeoffs, and explicit non-goals.
System redesigns fail without calibrated narrative
With systems redesign, narrative should be meticulously calibrated per audience. Concerns must be contained, to enable feedback instead of panic. Mistaking resistance for misunderstanding slows progress and costs trust. I learned to be deliberate about where to hold firm, where to adapt, and how to sequence decisions.

